

Fig.1 Left ventricular hypertrophy ECG
ECG with left ventricular hypertrophy (LVH) is the most significant predictor of false-positive STEMI activations. ECG with LVH represents 18% of all STEMI alarms. This small American retrospective study analyzed the correlation between specific features of ECG with left ventricular hypertrophy and the presence of a culprit lesion on angiography in patient presenting with chest pain where STEMI alarm was activated. Among ECG with hypertrophy (Cornell or Sokolow-Lyon criteria, or R-wave amplitude >11 mm in lead aVL), an ST elevation of more than 25% of QRS peak to nadir amplitude and [presence of STE in 3 contiguous leads or presence of T-wave inversions in the anterior leads] (see table) had the same sensitivity than classic STEMI criterion but had a much higher specificity (91% versus 58%) to detect coronary occlusion in presence of LVH. This algorithm reduces false positive by 35%, sparing unnecessary catheterization laboratory activation. Future studies should test these criteria in diverse patient populations and in a prospective manner.
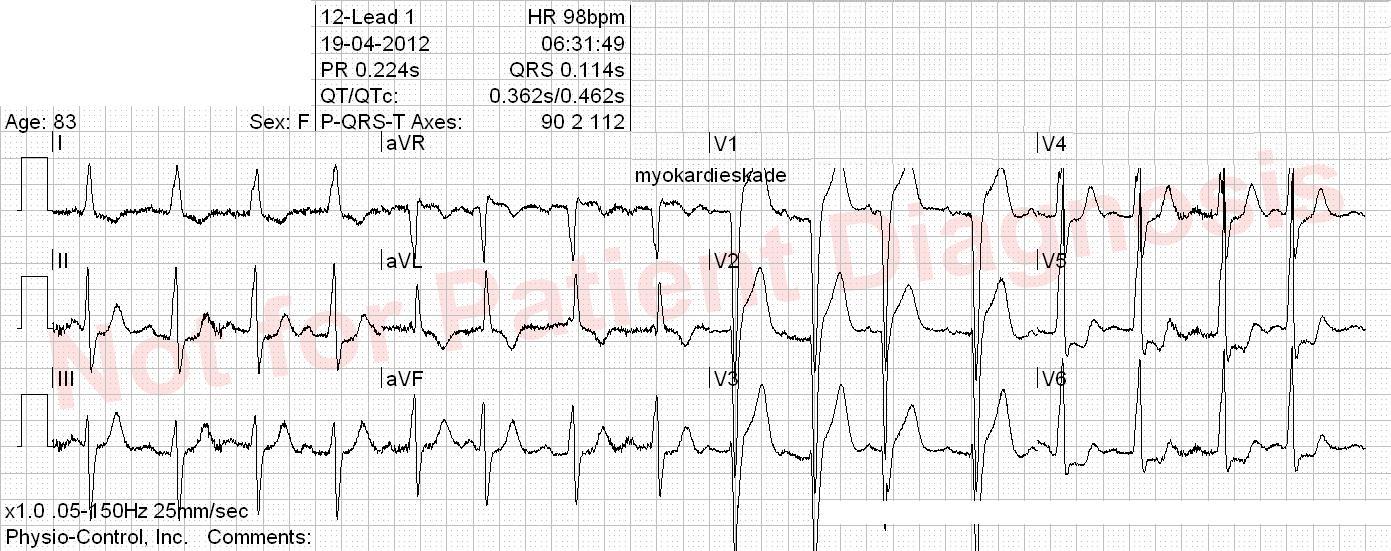
Fig.2 Is there a coronary occlusion in presence of left ventricular hypertrophy?

Ref. Armstrong et al. – Electrocardiographic Criteria for STEMI in Patients With LV Hypertrophy